Sleep Study

Full coverage
of your needs
SAS Sleep Apnoea Syndrome is a serious sleep-related breathing disorder that disrupts both sleep architecture and daytime quality of life, causing excessive daytime sleepiness. It is a highly prevalent condition, estimated to affect approximately 5% of the general population. It is classified into obstructive, central, and mixed types.
An apnoea is defined as a complete cessation of airflow lasting ten or more seconds, while hypopnoea is defined as either: a reduction in airflow of ≥50% for 10 or more seconds during sleep, accompanied by an oxygen desaturation of >3% and/or an arousal; or a reduction in airflow of ≥30% for 10 or more seconds, accompanied by an oxygen desaturation of >4%. These events must recur regularly throughout sleep despite continued inspiratory effort. Sleep Apnoea Syndrome is diagnosed when the Apnoea–Hypopnoea Index (AHI) exceeds 5 events per hour of sleep, and is classified as: mild (AHI: 5–15), moderate (AHI: 15–30), or severe (AHI: >30).
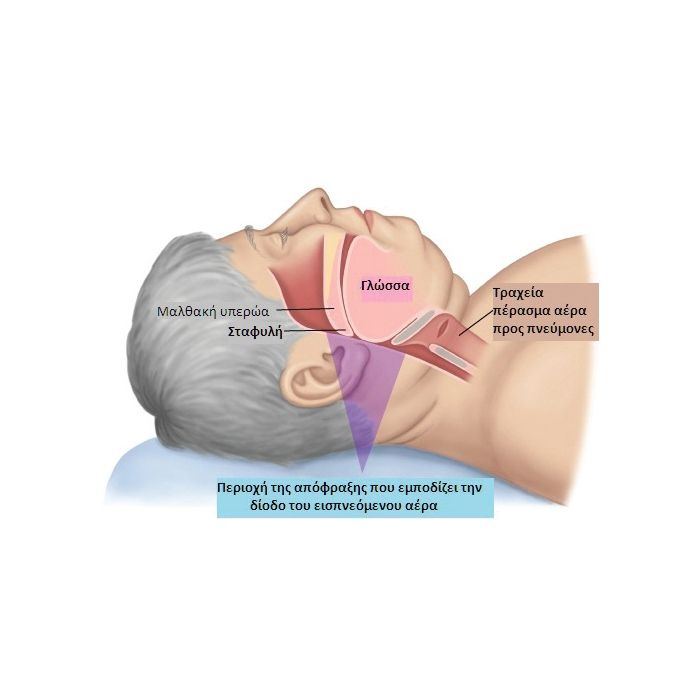
Obstructive sleep apnoea the most common form ,causes a fall in systemic oxygen saturation, which acts as an alarm signal to the brain. The brain responds by sending a command to the pharyngeal muscles to contract, thereby reopening the airway and allowing the patient to take an inspiratory breath (and thus receive oxygen), which is frequently accompanied by an audible sound — snoring. The muscles then relax again due to sleep, and this cycle repeats numerous times throughout the night.
During sleep, bed partners frequently report witnessed apnoeic pauses, loud snoring, restless sleep, and increased motor activity. Patients may complain of nocturia, sudden awakenings with a sensation of dyspnoea, choking, or suffocation — phenomena that interrupt and fragment normal sleep continuity.
Upon waking, patients commonly report non-restorative sleep, persistent fatigue, and excessive daytime sleepiness — symptoms with significant consequences for quality of life. Daytime sleepiness is the cardinal symptom of SAS and results from poor sleep quality due to sleep fragmentation by conscious or unconscious arousals. Associated manifestations may include irritability, anxiety disorder, reduced libido, and depression.
Serious life-threatening risks associated with untreated obstructive sleep apnoea include:
- arterial hypertension, resistant to medication.
- acute myocardial infarction - coronary heart disease
- vascular stroke
- cardiac arrest
- sudden death
- arrhythmias
- Insulin resistance and association with Diabetes Mellitus and/or metabolic syndrome & Increased risk of road traffic accidents due to excessive daytime sleepiness
Predisposing factors include obesity, the most significant risk factor in middle-aged adults, congenital or acquired craniofacial and cervical anomalies, menopause, and endocrinological disorders. Smoking and, particularly, alcohol consumption exacerbate sleep-disordered breathing episodes. In children, the primary risk factor is adenotonsillar hypertrophy.
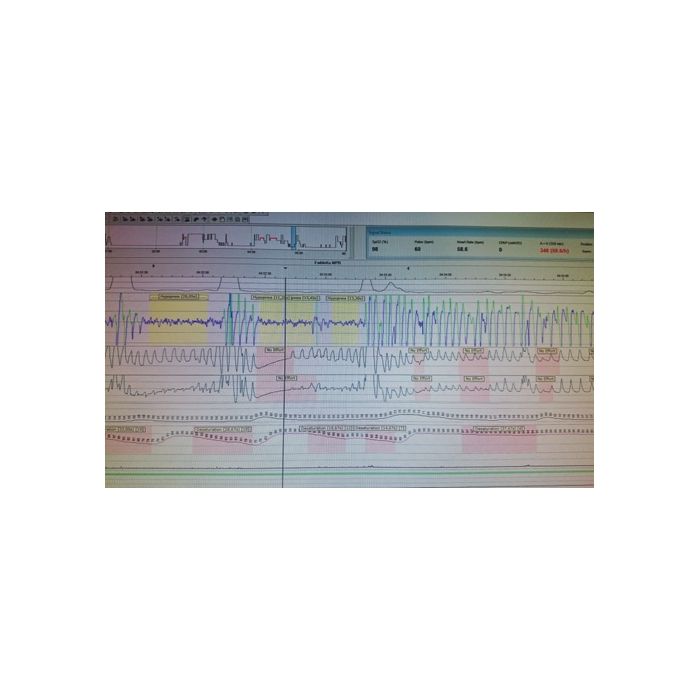
SYA diagnosis: is done with the very logical sleep study in a sleep laboratory.
Addressing SAY:
- Conservative measures: weight loss, avoiding alcohol and sedative drugs, avoiding supine sleeping position, treating nasal congestion.
- It is applied at all stages of severity, but especially in mild SARS.
- Surgical restoration by an ENT doctor (staphyloperiodopharyngoplasty), dental prostheses. Applied in limited cases,
- Nasal Continuous Positive Airway Pressure (nCPAP): the most widely applied treatment, particularly for moderate-to-severe obstructive SAS.
Pharmacological management of persistent daytime sleepiness with modafinil. Reserved for limited cases and as an adjunct to other treatment modalities.
It should be noted that obstructive sleep apnoea also occurs in children (affecting approximately 1–2% of the general paediatric population). Diagnosis and management in this age group are undertaken by paediatricians with specialist expertise. Suspicion should be raised when a child presents with excessive daytime sleepiness at school, difficulty concentrating, or memory impairment — as reported by a parent or teacher.
Indications for sleep study referral:
- Patients with symptoms or signs of sleep apnoea, including snoring, witnessed apnoeic episodes (reported by a bed partner), sudden nocturnal awakenings, sleep fragmentation, excessive daytime sleepiness and fatigue, and impaired concentration and/or memory. In particular, patients with heavy snoring combined with marked daytime sleepiness and/or witnessed apnoeas.
- Patients with chronic respiratory disease (e.g. COPD) and concurrent right heart failure, polycythaemia, or hypercapnic respiratory failure disproportionate to the degree of pulmonary impairment — especially those with coexisting cardiovascular disease or safety-critical occupations (requiring a high level of sustained attention and concentration).
- Patients with neuromuscular disease or thoracic wall deformity, particularly when diurnal hypercapnia or signs of pulmonary hypertension are present, as these patients are at high risk of developing severe alveolar hypoventilation during sleep.
- Professional drivers, in accordance with Greek Government Gazette 2734B/16 December 2015 (No. A3/71537/10872 — transposition of EU Directive 2014/85/EC of 1 July 2014, amending Directive 2006/126/EC of the European Parliament and of the Council on driving licences).
Sleep Study Coordinator
Daenas K. Christos Pulmonologist – Phthisiologist (Tuberculosis Specialist)